Epiretinal membrane (ERM) peel
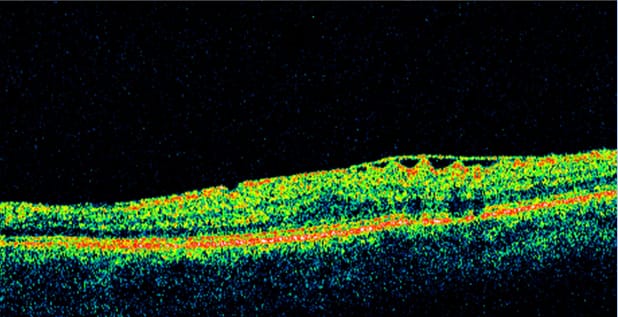
ERM: Fibrocellular proliferation on the inner retinal surface (ILM) causing macular pucker, thickening, and distortion.
Indications for surgery:
Symptomatic metamorphopsia, decreased VA (e.g., ≤20/40–20/60), tractional distortion on OCT.
Surgical Approach (Often with PPV)
- 25/27-g PPV
- Stain with Brilliant Blue G (BBG) ± ICG (use cautiously) to visualize ILM
- Initiate flap with pick/forceps
- Peel ERM (± ILM) 360° around fovea
- Avoid direct trauma at foveal center
- Fluid-air exchange optional
- Gas typically not required unless concomitant pathology.
- Many uncomplicated ERM peels end with air (short tamponade) or even BSS; long‑acting gas rarely needed unless combined with other pathology.
ILM Peel or Not to Peel?
- ERM+ILM peel reduces recurrence but may increase microstructural changes; many surgeons peel ILM routinely.
- Fovea-sparing ILM approaches are used in selected scenarios (e.g., myopic foveoschisis), not typical ERM.
OCT Prognostics
Outer retinal integrity (ellipsoid zone), baseline VA, and symptom duration predict outcomes. Typical gain: ~1-2 Snellen lines over months; persistent metamorphopsia possible.
Most patients gain lines of vision and reduced metamorphopsia; recovery can take months; worse baseline photoreceptor integrity → worse final VA. Monitor for cataract (if phakic), CME, and rare macular hole.
Complications
CME, small paracentral scotomas, MH formation (<~1-2%), retinal tears/RD, cataract progression (if phakic), IOP spikes, endophthalmitis.