Retinal Detachment (RD) Repair
What is RD
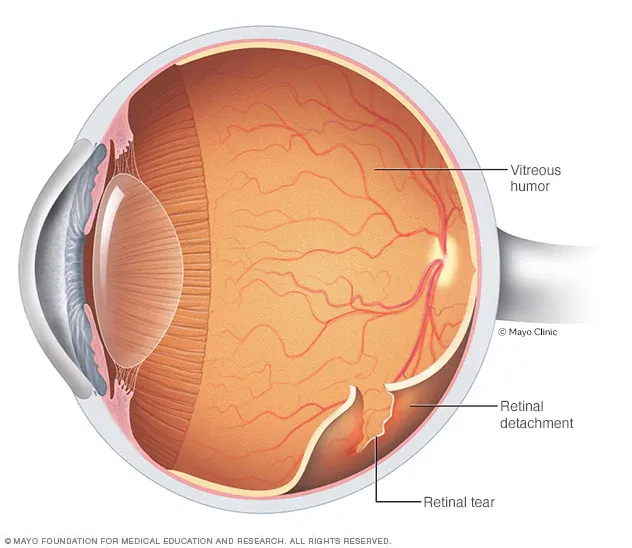
- Rhegmatogenous RD: Separation of neurosensory retina from the RPE due to a full-thickness retinal break that allows liquefied vitreous to enter the subretinal space.
- Risk factors: lattice degeneration, PVD with traction, high myopia, prior surgery/trauma, aphakia/pseudophakia.
- Exudative RD: Subretinal fluid from choroidal/retinal vascular leakage (e.g., inflammatory, neoplastic). No break.
- Tractional RD: Retinal elevation from fibrovascular membranes exerting traction (e.g., PDR, ROP).
Treatment Goal: close all retinal breaks and achieve chorioretinal adhesion (laser/cryotherapy) while neutralizing vitreoretinal traction.
Core Surgical Options
- Pneumatic Retinopexy (PR): In-office gas bubble + retinopexy (cryotherapy/laser).
- Best for one or few superior breaks in mobile retina, cooperative patient, no significant PVR.
- Scleral Buckle (SB): External indentation using silicone elements to support breaks and reduce vitreoretinal traction
- Ideal for young phakic, anterior/inferior pathology, small atrophic holes, round holes, and no PVD.
- Pars Plana Vitrectomy (PPV): 23/25/27-gauge microincisional vitrectomy to remove traction, identify/laser all breaks, and provide
internal tamponade (gas or oil).- Often combined with SB for PVR, inferior breaks, dialysis, or giant retinal tears (GRT).
Key Steps in PPV for Rhegmatogenous RD
- Mark sclerotomy sites (3.5–4.0 mm posterior to limbus depending on lens status).
- Core vitrectomy → induce/complete PVD.
- Shave vitreous base with scleral depression.
- Identify and treat all breaks (endolaser/cryotherapy).
- Drain SRF via break or posterior retinotomy (assisted by perfluorocarbon liquid if needed).
- Fluid–air exchange.
- Internal tamponade selection (SF6/C3F8/C2F6 or silicone oil).
- Sclerotomy closure as needed.
When to Add a Buckle to PPV?
- Inferior pathology
- Extensive lattice with multiple small holes;
- Young phakic eye with strong vitreous base traction
- Dialysis
- GRT edge support
- Early PVR
Postoperative Positioning (General Principles)
Position such that the tamponade bubble contacts the break(s).
- Superior breaks: head upright or slight face-down
- Macula-off with posterior breaks: strict face-down early
- inferior breaks: face-down or specific side-tilt
- Silicone oil less position-sensitive but still advisable initially.
Complications
CME, ERM, recurrent RD (missed break/PVR), choroidal detachment/effusion, hypotony, IOP spikes, endophthalmitis, cataract progression (in phakic eyes), diplopia with SB, myopic shift from SB